
The Relational Nature of TA, Sensorimotor Psychotherapy, DBR, and ILF Neurofeedback
/Introduction
Sometimes therapy approaches are described in ways that make them sound quite separate from one another.
Transactional Analysis (TA) may be seen as a relational and psychological model.
Sensorimotor Psychotherapy (SP) may be thought of as body-based.
Deep Brain Reorienting (DBR) may be understood as a trauma-processing method focused on shock and threat.
ILF neurofeedback may be seen as a form of nervous system training.
Yet in practice, all four can be understood as deeply concerned with relationship.
Not relationship in a narrow or simplistic sense, but in a fuller one: how human beings are shaped in contact with others, how safety and danger are learned relationally, how the self develops in relationship, and how healing often depends on what becomes possible within relationship too.
Although they differ in language and emphasis, TA, SP, DBR, and ILF neurofeedback can all be part of an approach that recognises that emotional life is not formed in isolation. Our patterns of feeling, responding, anticipating, protecting, and making meaning are profoundly influenced by early and ongoing relational experience.
Relationship is not an extra in therapy
It can sometimes be tempting to think of relationship as one aspect of therapy among many.
But for approaches such as TA, SP, and DBR, relationship is not an optional extra added on top of technique. It is woven into the whole understanding of how distress develops and how change becomes possible. And while ILF neurofeedback is not a relational therapy in itself, it can still support the nervous system conditions that make relational contact easier to sustain.
Human beings are born into relationship. We regulate, organise, and survive through relationship. We come to know whether the world feels welcoming, overwhelming, unpredictable, shaming, attuned, intrusive, or absent largely through relationship.
This means that many struggles brought to therapy are not simply “symptoms” sitting inside an isolated individual. They often reflect ways the person has had to organise around attachment, misattunement, protection, adaptation, shock, and survival in contact with others.
That is where these approaches meet in an important way.
TA: a relational understanding of self and contact
At its best, Transactional Analysis is far more than a set of concepts or diagrams. It is a profoundly relational way of understanding how people come into contact with themselves and others.
TA recognises that our ways of relating are patterned. We carry expectations, internalised relational experiences, and learned responses into present life. We may long for closeness while fearing it. We may seek recognition while defending against exposure. We may find ourselves caught in familiar transactions that repeat something older, often without fully realising it.
The TA model of Parent, Adult, and Child ego states offers one way of understanding this. Ego states are not separate personalities, but distinct patterns of feeling, meaning, bodily organisation, and behaviour. They help us see that we do not always respond from the same place within ourselves, and that different aspects of our experience may be activated in different relational moments.
In a relational TA frame, this is not only about analysing the client from a distance. It is about attending to what happens between therapist and client. The therapeutic relationship becomes a place where old expectations, adaptations, anxieties, and defences may become visible. Not to shame or expose the person, but to understand more deeply what they have had to organise around in order to survive and remain connected.
TA is deeply relational because it understands that selfhood is formed in relationship, and that therapeutic change often involves a new kind of relational experience rather than insight alone.
SP: the body as relational history
Sensorimotor Psychotherapy is often described as a body-oriented therapy, which is true, but that description can sound narrower than it really is.
SP is deeply relational because it understands that the body itself carries relational history.
Posture, tension, impulse, orientation, movement, collapse, bracing, reaching, holding back, going still — these are not only physical events. They are often part of how a person learned to manage contact, danger, closeness, helplessness, protest, submission, or the absence of attunement.
A person may lower their gaze without knowing why.
They may tense when someone is kind to them.
They may smile while feeling distressed.
They may freeze when they want to speak.
They may move towards others and away from themselves at the same time.
SP helps bring careful attention to these embodied patterns, not as abstract bodily phenomena, but as meaningful expressions of lived and often relational experience.
In this sense, SP does not move away from relationship when it attends to the body. It often moves closer to it. It asks: How has relationship been held in the body? What was interrupted? What had to be inhibited? What protective responses became necessary? What was never able to complete, express, or settle?
SP is relational because it understands that the nervous system and the body are shaped in interaction with others, and that healing often requires an experience of enough safety, tracking, pacing, and attunement within the therapeutic relationship.
DBR: shock, orienting, and relational threat
Deep Brain Reorienting is sometimes described mainly in neurophysiological terms, but it too is deeply relational in its implications.
DBR pays close attention to the sequence through which shock and threat are processed, including orienting, tension, shock, and affect. This can be especially important where a person’s difficulties are rooted in experiences that overwhelmed the system before they could be fully processed.
Many of these experiences are relational.
They may involve obvious trauma, but also moments of sudden emotional injury, alarm, rejection, intrusion, humiliation, misattunement, or terror in the presence of another person. Sometimes what becomes deeply organised in the nervous system is not only the event itself, but what happened in relationship at that moment — who was there, who was not there, who turned away, who became frightening, who failed to protect, who could not receive what was needed.
DBR helps access these deeply rooted shock states carefully and gradually. In doing so, it often reveals just how relational trauma can be. The pain is not only about what happened to the person as an isolated individual. It is often about what happened in the space between self and other, at moments where safety, attachment, or recognition were ruptured.
DBR is also relational in another sense: the work depends heavily on careful pacing, attunement, and containment. The therapist’s presence matters. Too much pressure, speed, or interpretive intrusion can disrupt the process. The work asks for a high degree of respect for the person’s system and for the unfolding of experience.
That, too, is relational.
ILF neurofeedback: supporting the conditions for grounded attunement
Alongside explicitly relational therapies, ILF neurofeedback can also play an important supporting role.
It is not a relational psychotherapy in itself, and it does not replace the importance of the therapeutic relationship. What it may do, however, is help support greater nervous system stability, reducing the degree to which a person remains caught in hyperarousal, shutdown, vigilance, or rapid stress reactivity.
For some people, this can have important relational implications. When the nervous system is less dominated by threat and better able to settle, it may become easier to stay present with another person, to register cues of safety more accurately, and to tolerate contact without becoming so quickly overwhelmed or defended.
In this sense, ILF neurofeedback may help facilitate the system’s capacity for attunement from a place of groundedness and safety. It does not create relationship on its own, but it may help make relational presence more available.
For people whose systems have been organised around chronic stress, trauma, overwhelm, or instability, this kind of support can sometimes make other therapeutic work more accessible. Reflection may become easier. Contact may feel less threatening. The body may become less preoccupied with danger and more available for connection. All this means that one develops more capacity to attend the psychotherapeutic process.
Different languages, shared truths
TA, SP, DBR, and ILF neurofeedback do not say exactly the same thing.
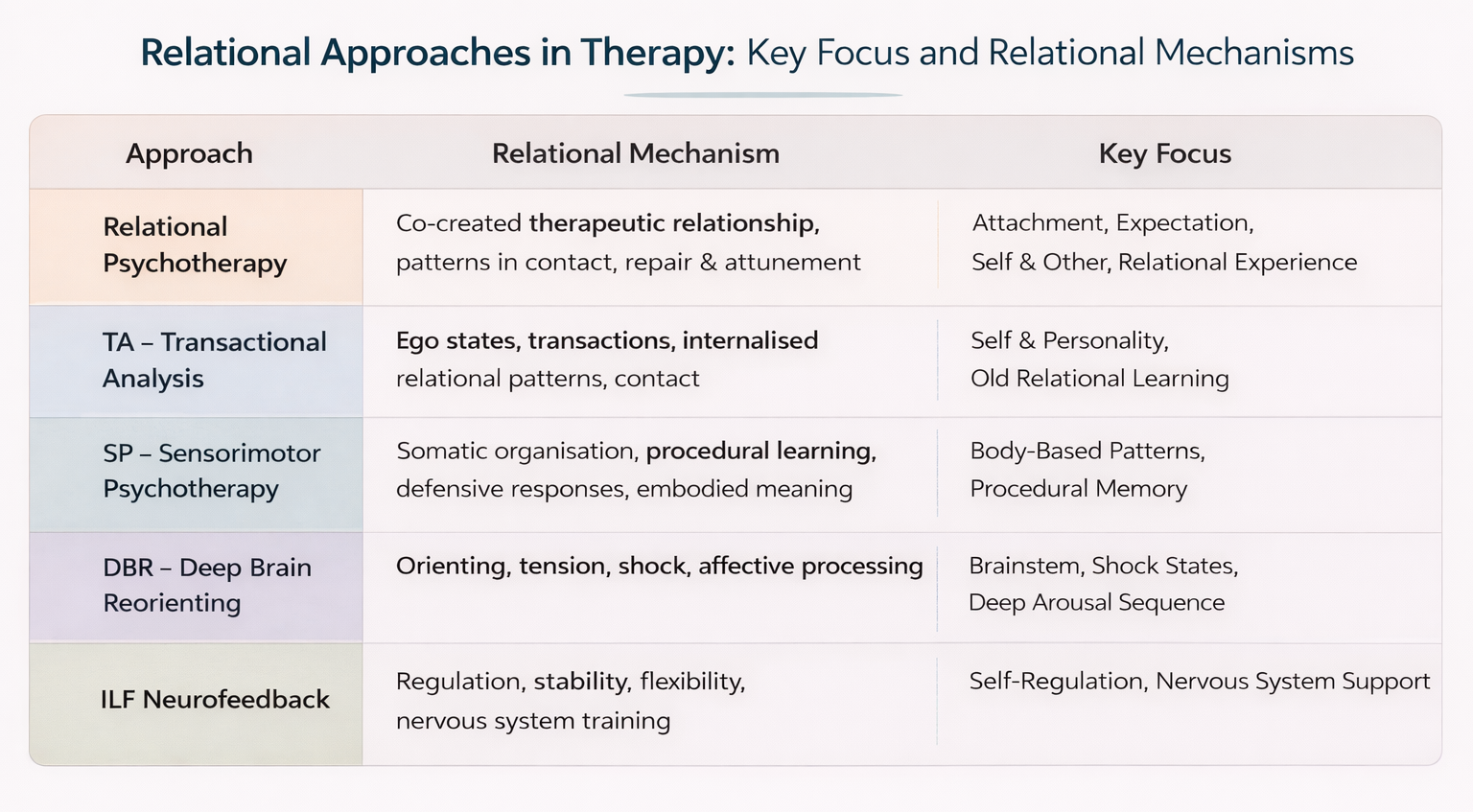
TA may speak more in terms of ego states, transactions, internalised relational patterns, and contact.
SP may speak more in terms of somatic organisation, procedural learning, defensive responses, and embodied meaning.
DBR may speak more in terms of orienting, tension, shock, and affective processing.
ILF neurofeedback may speak more in terms of regulation, stability, flexibility, and nervous system training.
But underneath these different languages, there are shared truths.
All recognise that:
People are shaped by relationship.
Distress is often organised through relationship.
Old patterns may become active in present relational contexts.
The body and nervous system are involved, not just thought.
Insight alone is often not enough.
Therapeutic change depends not only on technique, but on attunement, pacing, and the quality of contact.
ILF neurofeedback adds a further dimension by helping support the regulatory stability that can make relational contact, attunement, and embodied presence easier to sustain.
This is one reason these approaches can complement each other so well.
Why this matters in practice
When therapy takes the deeply relational nature of experience seriously, it can begin to hold together things that are often split apart.
A person may need help understanding their ego states and relational patterns.
They may also need help noticing how those patterns are carried in posture, tension, impulse, and autonomic response.
They may also need support in approaching shock and affect that sit beneath their more familiar reactions.
And they may benefit from support for the nervous system stability that makes reflection, contact, and attunement more possible.
If only one layer is addressed, something important may be missed.
A person may gain insight but still feel hijacked by their nervous system.
They may work somatically but without enough meaning or relational context.
They may process trauma without sufficiently understanding how present relationships continue to activate old expectations.
Or they may understand the work well, yet remain too physiologically dysregulated to stay grounded in it.
An integrative approach can help these layers speak to one another.
TA can help name the patterns of self and relationship.
SP can help track how those patterns live in the body.
DBR can help address deeper shock-based organisation that keeps certain responses locked in place.
ILF neurofeedback can help support the regulatory stability that makes relational contact, attunement, and embodied presence easier to sustain.
Held within a genuinely relational therapeutic frame, this can support not only understanding, but deeper integration.
Therapy as a new relational experience
Perhaps one of the most important things these approaches share is that they do not treat healing as a purely intellectual task.
Therapy is not simply a place to think about oneself more accurately. It can also become a place where a person gradually experiences something different in relationship.
That may include:
Being met with steadiness rather than pressure.
Being understood without being overrun.
Being able to notice bodily responses without shame.
Having affect approached without fear or force.
Recognising old expectations as they arise in the room.
Discovering that contact can sometimes remain possible even in the presence of vulnerability.
This does not mean therapy becomes idealised or perfect. Rupture, uncertainty, misunderstanding, and limitation can all be part of therapeutic work too. But in a relational approach, these are not treated as irrelevant or to be avoided at any cost. They may become part of what can be noticed, understood, and sometimes repaired.
That process can be deeply transformative.
A closing reflection
To say that TA, Sensorimotor Psychotherapy, DBR, and ILF neurofeedback are deeply relational is not just to say that they all value empathy.
It is to say something more fundamental: that they each understand human suffering and healing as shaped by relationship at multiple levels — psychological, embodied, developmental, and neurophysiological.
They recognise that what we carry is often not only belief or memory, but organised relational experience: in our expectations, our protective strategies, our bodily responses, our shock patterns, and our capacity for contact.
And they each, in their own way, point towards the same hope: that through sufficiently careful, attuned, embodied, and thoughtful therapeutic work, what was shaped in painful relationship need not remain fixed forever.
If this way of working resonates with you, you may also wish to explore: